The Impact Of Back Pain In The UK
Almost half of the adult population in the UK suffer with low back pain lasting for at least 24 hours at some time in the year according to the charity BackCare. In 2013, 31 million sick days were lost in the UK for back pain according to the Office for National Statistics, and about 8 in 10 people in the UK suffer at least one bout of low back pain in their lives according to www.patient.co.uk.
So you can see there is a huge effect on the economy and quality of life for many individuals. Many people are diagnosed with the umbrella term of ‘mechanical back pain’ which could be one structure or a combination of structures causing their problem. Many people are diagnosed with the umbrella term of ‘mechanical back pain’ which could be one structure such as a disc, or a combination of structures such as a disc and a muscle causing their problem. The key thing to take away though is that the different structures work as a team, so the original injury and/or compensations which occur after can lead to pain and discomfort.
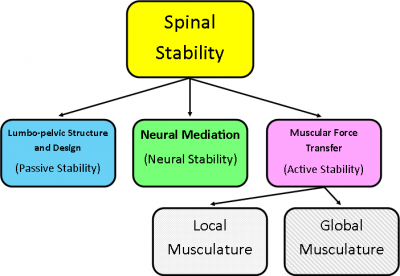
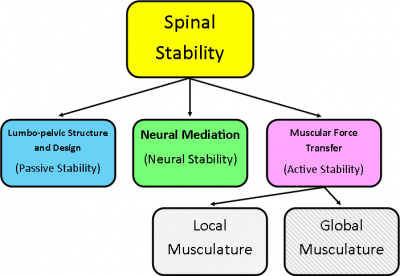
One of the leading theories regarding this teamwork is of Panjabi (1992) which although 23 years old is still referenced frequently, it separates the spinal anatomy into 3 subsystems, and shows how all three subsystems affect each other and can compensate for each other as needed. However long term adaptation or compensation will lead to altered optimal stabilisation around the spine, which could also lead to back pain.
The human spine
To look at this from a different angle, let’s look at the anatomy of the human spine in more detail:
The spine is made up of 33 vertebrae, 24 articulating ones and 9 fused ones to make the sacrum and coccyx. 23 Discs and many muscles, ligaments and fascial connections, never mind the spinal cord and nerves! So why do we have so many joints and discs? It’s so we can move easily in different direction, have dynamic control and the discs offer a suspension system for the whole body.
To zoom in further still, you can see below there is very little space available at the spinal segments for swelling or a disc to bulge without causing some compression of a nearby structure.
In this article we are going to look closer at the discogenic causes of back pain (part of the passive subsystem according to Panjabi, 1992) and thus what type of mattress should help.
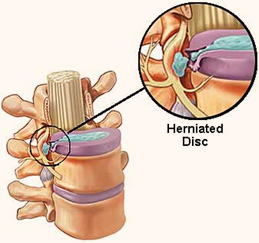
Some of the frequently used terminology to describe disc damage include; prolapsed disc, herniated disc, disc protuberance or bulge, ‘slipped disc’, degenerate, dehydrated or dessicated discs. The above picture shows an example of the first 5 terms. Disc damage can occur at any level in the spine, but is most common in the lumbar spine.
Discs are like any other soft tissue in the body, and can repair and heal themselves given the right environment and time. But unfortunately not all do, especially if the damage to the disc was initially more significant. Hence people require surgery for more severe disc injuries, especially when the individual has significant amounts of referred pain / nerve pain (radiculopathy) or a motor weakness due to neural compression either at the nerve or spinal cord, causing symptoms like foot drop or bladder and bowel dysfunctions.
With disc injuries in mind the majority of clients with back pain tend to find a medium/firm to firm mattress (Winter, 2006) or a firm mattress topped with a memory foam topper helps to increase their comfort and reduce their pain. But the benefits of different beds can depend on the direction of the disc bulge/prolapse and also the favoured sleeping position. Most discs bulge backwards (posterior) or sidewards (laterally) or a combination of both (posteriorlaterally).
Choosing a bed to manage back pain
Classically, lying on one’s stomach can help with discogenic pain, as it helps push the contents of the disc forwards and away from the tear site in the wall of the disc, but this doesn’t apply to everyone. Stomach sleepers tend to like a medium firm mattress as too much firmness can result in increased pressure on the knees and chest, and a softer mattress can allow the client to sink too deeply causing excessive extension at the spinal joints pushing the facet joints together and potentially causing discomfort, and misalignment at the neck and head.
Side sleepers tend to prefer medium to soft firmness of the mattress, as the pressure is more focused on the shoulders and hips which have a smaller surface area. Some tend to also enjoy a medium to firm mattress with a memory foam topper, or popping a pillow between the legs to reduce the twist at the back.
Back sleepers tend to prefer medium to firm firmness as they have a larger surface area in contact with the bed, so like the support. However a back sleeper with a facet joint dysfunction at the spine would not necessarily enjoy that mattress as it will potentially promote extension through the spine which could increase their pain, so again a memory foam alternative may work to cushion the spine or pillows under the knees to take the load off the low back area.
Facet joint dysfunction, articular issues and neural causes of spinal pain will be discussed in the next article, relating the anatomy and structure to the best solutions for a great night’s sleep. Until next time, sleep well….
Download Your Free Brochure
Revival Beds collection of quality mattresses, wooden bed frames and bedroom furniture are all handmade to order in the UK from the finest materials. To find out more, simply click on the link below to download your free brochure.
References
The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. Panjabi MM J Spinal Disord. 1992 Dec;5(4):383-9; discussion 397.
Subjective rating of perceived back pain, stiffness and sleep quality following introduction of medium-firm bedding systems. J Chiropr Med. 2006 Winter; 5(4):128-34.